New Knowledge, Innovations, and
Improvements
Magnet hospitals and their employees have a responsibility to contribute to patient care, the organization, and the profession in terms of new knowledge, innovations, and improvements. Utilizing research and evidence-based practice (EBP), gives me the opportunity to change policies, patient care, and outcomes. By doing so, New knowledge, Innovations and Improvements occurs.
The FOCUS-PDCA model helps improvement teams focus on processes rather than just the individuals. It encourages teamwork and shared ownership of the improvement opportunity. I performed a FOCUS-PDCA on the labeling process that I presented as a PowerPoint to the QSA regarding the labeling process being used on the MS PCU.
Since noticing the increase in laboratory specimen errors on the MS PCU, I decided to improve the quality of care that we provide our patients on MS PCU and throughout the hospital. By writing employee numbers on every specimen label that goes to the clinical lab, this ideally would help in the reduction of errors that occur on the unit.
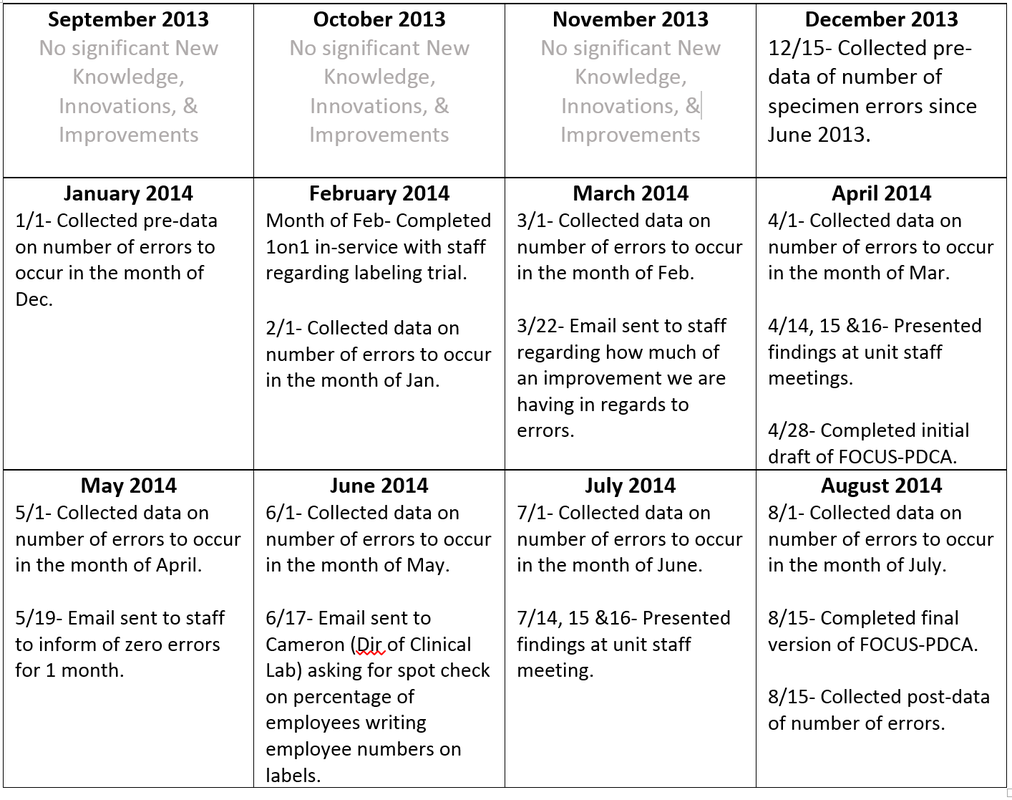
I began by tracking the amount of errors that occurred on the MS PCU that were reported by the clinical lab by way of Safety Intelligence (SI) reports. I looked at the number of errors that we presented with prior to the initiation of the improvement. This began in June 2013 after the MS PCU opened on AIP.
After I initiated the improvement, I remained keeping track of all SI's that were reported by the clinical lab. I kept the staff well informed of the amount of errors during this process by way of emails, face-to-face communication, and staff meetings.
After a few months of the process change and seeing a slight reduction of specimen errors, I along with the sub-committee laboratory task-force joined forces and developed the Orange Card that will help in the reduction of extra labels being added to the specimen bag.
As part of the Labeling Campaign that went hospital wide, Tyler Smith, editor and writer for The Insider interviewed the sub-committee task-force and myself to publish information in an article within the paper. This was posted onto the HUB in the July 8th 2014 edition.
Since noticing the increase in laboratory specimen errors on the MS PCU, I decided to improve the quality of care that we provide our patients on MS PCU and throughout the hospital. By writing employee numbers on every specimen label that goes to the clinical lab, this ideally would help in the reduction of errors that occur on the unit.
I began by tracking the amount of errors that occurred on the MS PCU that were reported by the clinical lab by way of Safety Intelligence (SI) reports. I looked at the number of errors that we presented with prior to the initiation of the improvement. This began in June 2013 after the MS PCU opened on AIP.
After I initiated the improvement, I remained keeping track of all SI's that were reported by the clinical lab. I kept the staff well informed of the amount of errors during this process by way of emails, face-to-face communication, and staff meetings.
After a few months of the process change and seeing a slight reduction of specimen errors, I along with the sub-committee laboratory task-force joined forces and developed the Orange Card that will help in the reduction of extra labels being added to the specimen bag.
As part of the Labeling Campaign that went hospital wide, Tyler Smith, editor and writer for The Insider interviewed the sub-committee task-force and myself to publish information in an article within the paper. This was posted onto the HUB in the July 8th 2014 edition.
Timeline