Transformational Leadership

Transformational Leadership is a theory that was first introduced in 1978 by James MacGregor Burns. He describes this theory as a leader that engages others in a way that enhances their performance and motivation.
Transformational Leaders are often characterized by:
- Challenging a process
- Modeling the way
- Encouraging the heart
- Enable others to act
- Inspire a shared vision
I began my career with UCH as a travel nurse hired on the Cardiovascular Intermediate Care Unit (CVIMCU) on the 10th floor AIP. This unit went through some major changes in May 2013, when the CVIMCU was separated into two new specialty units. These units are the Medical Surgical Progressive Care Unit (MS PCU) and the Cardiac Progressive Care Unit (CPCU). I became a permanent staff member of the MS PCU in December 2013. I chose to become part of the team on the MS PCU due to the great team work, respect for one another, and feeling as if I had a home at UCH.
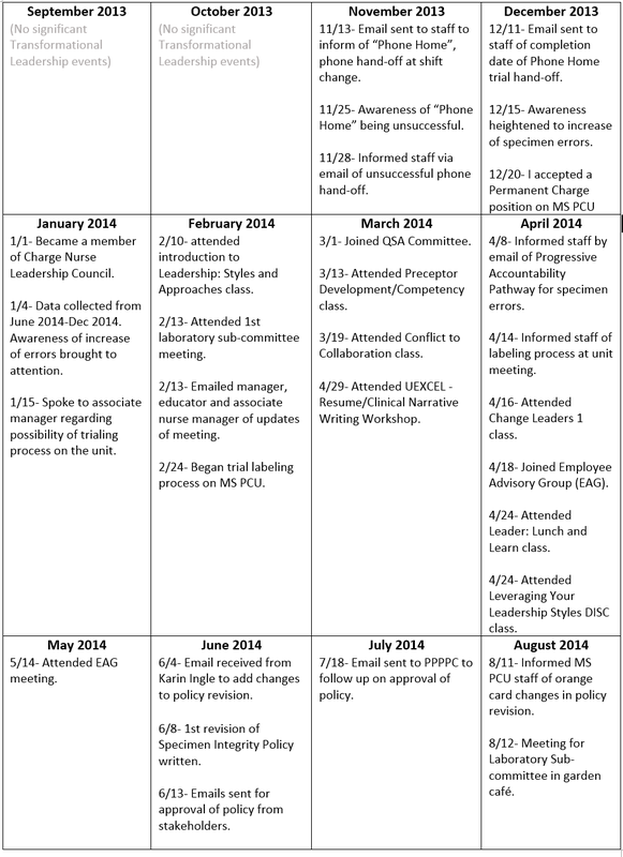
Shortly after the formation of the 10th floor into the newly formed MS PCU, we began to settle in and create a home. I began to notice some small things that were appearing to make the work day a little less smooth. My first attempt at a unit improvement project was to attempt to make a smoother transition from shift to shift with regards to handing off the Cisco phones. Many phones were becoming lost or misplaced and some were taken home accidentally by staff. I developed a solution to the problem of the misplaced phones and made a "Phone Home". This involved placing the phones on the docking station prior to leaving for the shift and picking them up when you began your shift. As you'll see, this was not very successful.
As I transitioned from the role of Relief Charge Nurse to Permanent Charge Nurse in December 2013, I became more involved in improving the quality and safety of care our patients received. I began to notice a trend of increasing specimen errors on our unit. As a unit, we oriented over 60 new employees, including Registered Nurses (RN's), Certified Nursing Assistants (CNA's), and Advanced Care Partner's (ACP's) from April 2013 to November 2013. At first, I suspected the increase of errors may have been due to the learning curve of so many new employees. As time passed and I still did not see a significant decrease in the amount of errors, I knew that something had to change in our specimen collection practice. I wanted to be the one to initiate this change on MS PCU as I had a strong passion for improving the quality of care and safe care that our patients receive on a daily basis.
Committees are an important part of being an active member of a unit and hospital. I have chosen to be a part of the Quality Safety Advocates (QSA), Charge Nurse Leadership Council and Employee Advisory Group (EAG). In doing so, it has given me a sense of ownership to my unit and hospital.
Keeping policies and procedures up-to-date with evidence based research and best practice is an essential part to providing the best possible care to our patients. As part of my labeling process changes, I revised the policy Specimen Integrity and presented it to the Professional Practice Policy & Procedure Committee (PPPPC) in which it was approved.
Shortly after the formation of the 10th floor into the newly formed MS PCU, we began to settle in and create a home. I began to notice some small things that were appearing to make the work day a little less smooth. My first attempt at a unit improvement project was to attempt to make a smoother transition from shift to shift with regards to handing off the Cisco phones. Many phones were becoming lost or misplaced and some were taken home accidentally by staff. I developed a solution to the problem of the misplaced phones and made a "Phone Home". This involved placing the phones on the docking station prior to leaving for the shift and picking them up when you began your shift. As you'll see, this was not very successful.
As I transitioned from the role of Relief Charge Nurse to Permanent Charge Nurse in December 2013, I became more involved in improving the quality and safety of care our patients received. I began to notice a trend of increasing specimen errors on our unit. As a unit, we oriented over 60 new employees, including Registered Nurses (RN's), Certified Nursing Assistants (CNA's), and Advanced Care Partner's (ACP's) from April 2013 to November 2013. At first, I suspected the increase of errors may have been due to the learning curve of so many new employees. As time passed and I still did not see a significant decrease in the amount of errors, I knew that something had to change in our specimen collection practice. I wanted to be the one to initiate this change on MS PCU as I had a strong passion for improving the quality of care and safe care that our patients receive on a daily basis.
Committees are an important part of being an active member of a unit and hospital. I have chosen to be a part of the Quality Safety Advocates (QSA), Charge Nurse Leadership Council and Employee Advisory Group (EAG). In doing so, it has given me a sense of ownership to my unit and hospital.
Keeping policies and procedures up-to-date with evidence based research and best practice is an essential part to providing the best possible care to our patients. As part of my labeling process changes, I revised the policy Specimen Integrity and presented it to the Professional Practice Policy & Procedure Committee (PPPPC) in which it was approved.
This Component of Magnetism is truly understanding the role of nursing; the application of that role with patients, families, co-workers and interdisciplinary team. The goal of this component is more than just building and establishing my own professional practice; it is what my professional practice can achieve. I strive to improve the quality of care that the patients on MS PCU receive and decrease the risk of error to occur in the area of specimen collection.
A leader is one who knows the way, goes the way, and shows the way. —John Maxwell
Timeline